I've learned a bit of immunology from hanging out with immunologists so I'm going to try and explain how vaccines protect you from the worst consequences of an infection and why booster shots aren't as necessary as you think. This will be an illustration of how difficult it is for the media to keep you correctly informed about real science and why we should have more scientists explaining these things instead of doctors
Dozens of papers on this topic have been published over the past year or so and they all say the same thing. SARS-CoV-2 vaccinations induce an immediate production of antibodies in response to the spike protein antigen whether it's presented on the surface of a viral vector such as adenovirus or synthesized in your cells by mRNA. The antibodies are produced by a small number of B cells that just by chance happen to recognize the viral protein. These cells multiply rapidly so that within a few days you have enough antibodies being produced to fight off any infection.
Over time, the antibody production declines if there's no infection but some of the B cells become memory B cells that lie in wait for the next infection when they can be rapidly stimulated if you get infected months, or years, later. There's another type of cell called a T cell that also forms memory T cells that are very long-lasting and help fight off future infections.
Imagine that you encounter the virus several months after you've been vaccinated. As soon as the virus enters your body the memory cells are activated and the virus is attacked. You may have a mild case of COVID-19 for a few days but you are protected against the most severe forms of the disease. The point is that a reduction in antibody levels is perfectly normal. What's important is whether you have a robust level of memory B cells and memory T cells that can be activated. The hype in the media has convinced people that the vaccines are no longer effective after six months and you have to get a booster shot to protect you from COVID-19.
Here's a very recent paper that presents the data. It was published in Science on December 3, 2021.
Goel, R.R., Painter, M.M., Apostolidis, S.A., Mathew, D., Meng, W., Rosenfeld, A.M., Lundgreen, K.A., Reynaldi, A., Khoury, D.S. and Pattekar, A. et al. (2021) mRNA vaccines induce durable immune memory to SARS-CoV-2 and variants of concern. Science 374:eabm0829. doi: 10.1126/science.abm0829
Vaccination against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has proven highly effective at preventing severe COVID-19. However, the evolution of viral variants, and waning antibody levels over time, raise questions regarding the longevity of vaccine-induced immune protection. Goel et al. examined B and T lymphocyte responses in individuals who received SARS-CoV-2 messenger RNA vaccines. They performed a 6-month longitudinal study of individuals who never had SARS-CoV-2 infection compared with people who had recovered from SARS-CoV-2. Humoral and cellular immune memory was observed in vaccinated individuals, as were functional immune responses against the Alpha (B.1.1.7), Beta (B.1.351), and Delta (B.1.617.2) viral variants. Analysis of T cell activity suggested that robust cellular immune memory may prevent hospitalization by limiting the development of severe disease.
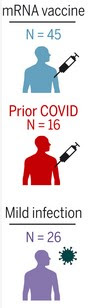
The authors looked at the immune reaction in three different groups. The first was the naive group of people who have never had COVID-19 but got the vaccine (blue). The second group was people who had already survived COVID-19 and then got vaccinated (red). The third group was composed of people who had mild cases of COVID-19 and never got vaccinated (purple).
This is a long paper with lots of experiments but the data can be summarized in the figure below. The authors looked at antibodies to the spike protein and to its specific ACE2 binding site. They also looked at neutralizing antibodies or the abiity of circulating antibodies to neutralize whole virus particles. The results are summarized in the first graph and they show that the antibody levels rise to maximum levels about one week after receiving the second dose of vaccine (administered four weeks after the first dose).
The antibody levels fall to about 10% of the maximum value over the next six months. (The x-axis is a log scale.) This is exactly what you expect for a typical vaccine. Note that the levels for people who had already been infected were higher to begin with but the rate of decline was similar to the naive group. This suggests that booster shots will have a similar effect on antibody levels.
The levels of memory B cells and memory T cells rise to a maximum at four months, right at the time of the second dose. They remain high at the end of six months.
Taken together, these data demonstrate that mRNA vaccines induced a population of memory B cells that was durable for at least six months after vaccinaton, and these cells were capable of rapidly producing functional antibodies against SARS-CoV-2, including neutralizing antibodies against VOCs [variants of concern], upon stimulation....
Taken together, these data indicate that mRNA vaccination generates durable SARS-CoV-2-specific CD4+ T cell memory in individuals who were not previously infected with SARS-CoV-2 and only transiently boosts these responses in SARS-CoV-2-recovered individuals.
What this means is described by the authors in the concluding remarks,
These data may also provide context for understanding potential discrepancies in vaccine efficacy at preventing infection versus severe disease, hospitalization, and death. Declining antibody titers over time likely reduce the potential that vaccination will completely prevent infection or provide near-sterilizing immunity. However, the durability of cellular immunity, here demonstrated for at least 6 months, may contribute to rapid recall responses that can limit initial viral replication and dissemination in the host, thereby preventing severe disease.
In other words, if you are fully vaccinated (two doses of mRNA vaccine) then you are well-protected against severe disease although you may suffer mild symptoms for a few days. You may be able to avoid the mild symptoms if you have gotten a recent booster shot but that effect is likely to decline in a few months.
The hype about booster shots is extremely misleading. The media is making it sound like all of your vaccine protection declines after six months and you need the boosters to have any chance at all against the omicron variant. How many times have you heard that your vaccine protection drops to 33% after six months?
You could argue that boosters aren't even necessary but that ignores the possibility that even a mild infection may be harmful to some people. It also ignores the possibility that by preventing even a mild infection you could be blocking the spread of the virus. I don't know of any data on viral loads after vaccination but I suspect that a booster offers some protection against spread.
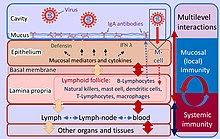
Image Credit: The coronavirus figure is from Alexy Solodovnikov and Wikmedia Commons.